






Barrett’s Oesophagus
Please click the questions below to reveal the answer
Barrett’s Oesophagus is a pre-malignant condition, in which the normal lining of the food pipe (oesophagus) changes to that found in the stomach, as a consequence of chronic reflux oesophagitis. Patients with Barrett’s have a 30-fold increased risk of developing oesophageal adenocarcinoma in comparison to the general population. However, only 1 in a 1000 patients with Barrett’s oesophagus will develop adenocarcinoma on an annual basis. Most people with Barrett’s oesophagus don’t have to worry, over 90% won’t develop oesophageal cancer in their lifetime.
Barrett’s oesophagus affects about 1-2% of the general population and 10% of those who report acid reflux symptoms.
Barrett’s Oesophagus results from chronic inflammation of the oesophagus secondary to reflux of stomach acid and other noxious substances. The reflux may or may not cause symptoms. The chronic inflammation then leads to the normal lining of the food pipe (squamous epithelium) to change to that found in the stomach (columnar epithelium). This change in the lining is termed Barrett’s Oesophagus. This is the body’s protective response to reduce inflammation as the stomach lining is much better at coping with acid exposure. Why Barrett’s Oesophagus develops in some patients with reflux and not in others remains unclear. However, research has identified male sex, white ethnicity, increased age and obesity as significant risk factors.
Barrett’s Oesophagus itself does not cause symptoms, however if you suffer with symptoms of gastro-oesophageal reflux disease (GORD) such as heartburn or volume reflux then you should ideally have an endoscopy for further assessment. Food getting stuck on swallowing and unexplained weight loss are red flags of possible cancer development in Barrett’s Oesophagus and therefore warrant urgent endoscopy.
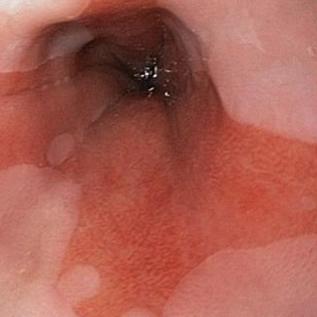
Upper Gastrointestinal Endoscopy is the gold-standard test for a diagnosis of Barrett’s Oesophagus. Diagnosis is based on visual confirmation of a change in the lining of the oesophagus and an accurate biopsy of the suspicious sites.
Decision for treatment is based on the presence of precancerous cells, termed dysplasia. This diagnosis is made by the histopathologist on examination of the biopsy specimens.
If dysplasia is present you will referred for consideration of Radiofrequency Ablation (RFA). This is an endoscopic treatment that burns off abnormal tissue using radio waves, which generate heat. Other techniques such as cryotherapy using liquid nitrogen to freeze diseased parts are also used. The aim of these treatments is to prevent the development of cancer in the future. If cancer develops and is detected in the Barrett’s oesophagus there may be an option for endoscopic resection if it is caught at a very early stage. Not everyone with Barrett’s oesophagus will develop dysplasia or cancer and therefore treatment is reserved for those that develop it.
If there is no dysplasia or cancer then Barrett’s Oesophagus can be treated with Proton Pump Inhibitors (e.g. Omeprazole, Lansoprazole). In a meta-analysis of nine studies including 5700 patients with Barrett’s Oesophagus, the use of daily PPI was associated with a trend toward a lower risk of oesophageal cancer. Some patients with Barrett’s oesophagus have severe reflux symptoms despite medication and may elect to have anti-reflux surgery.
Anti-reflux surgery is a useful option for highly selected patients with Barrett’s Oesophagus who appear symptomatically resistant to PPI treatment or have oesophageal inflammation which is resistant to PPI treatment. However, fundoplication has not been shown to be more effective than PPI treatment for preventing oesophageal adenocarcinoma in Barrett’s Oesophagus.
Guidelines suggests that an endoscopy with biopsies should be performed every two to three years for the purpose of surveillance. The aim of surveillance is to improve patient outcomes by detection of dysplasia or cancer at an early stage to ensure effective treatment
The best way to keep the lining of your oesophagus healthy is to address reflux symptoms. People with ongoing, untreated heartburn are much more likely to develop Barrett’s oesophagus. Untreated heartburn raises the risk of esophageal adenocarcinoma by 64 times. Other ways to decrease your risk factors include avoid drinking alcohol and smoking and maintain a healthy weight.